

Incivility You Cannot Ignore: How Nurse Educators Can Use Emotional Intelligence to Protect Learning and Patient Care
You probably know this scene.
It is 0630, and your clinical group has just arrived on the unit. One student waits near the nurses’ station while you hand out assignments. The nurse they are paired with looks at the list and says, “Oh, I have a student today,” with a tight smile and a quick sigh before turning and walking away.
Your student was already nervous. Now they stay close to the wall, wait to be told what to do, and decide not to ask the questions they had planned. Later, they tell you, “I did not want to bother her.”
This is just one example of incivility in nursing. It is subtle, easy to brush off, and powerful enough to shrink a learner in under thirty seconds.
What Incivility Looks Like Now
Incivility in nursing is often described as low-intensity, disrespectful behavior that violates norms of mutual respect. Eye-rolling, exclusion, belittling comments, sarcasm, or a cold tone can all communicate “you are a problem” even when the words do not say that out loud. One moment might seem small. Over time, they add up.
Recent work tracing the effects of nursing incivility shows that these behaviors are not harmless. They are linked to higher nurse stress, reduced patient engagement, and worse health outcomes, including readmissions and lower satisfaction (Alsadaan et al., 2024).
In nursing education and early practice, incivility often shows up in familiar ways: a preceptor who moves too fast and shows visible irritation when a new nurse asks for clarification, clinical staff who complain about “having another student today” within earshot, or faculty who correct a student in a way that shames more than it teaches. None of this appears in a competency checklist. Yet every one of these moments shapes how safe it feels to learn, to speak up, and to ask for help.
Why It Is Not Just A "Personality Clash"
It is easy to shrug and say, “That is just how she is,” or “They do not click.” The risk is that we turn a culture problem into an individual problem.
Incivility quietly touches three core areas of education and transition to practice.
Psychological safety and speaking up.
After a few bad interactions, students and new nurses often stop asking questions. They get very good at looking like they understand while they are still guessing. When people do not feel safe to say “I am not sure,” they are less likely to clarify, admit gaps, or call for help.
Professional identity and belonging.
Repeated messages like “We are too busy for students” eventually sound like “We are too busy for you.” Supportive, respectful environments help learners see themselves as needed and valued. Dismissive or hostile environments do the opposite and feed stories like “I am in the way” or “I am not cut out for this.”
Nurse well-being and patient outcomes.
Research has linked nursing incivility with higher nurse stress, emotional exhaustion, and worse patient outcomes, including lower engagement and more readmissions (Alsadaan et al., 2024). It also contributes to nurses showing up physically present but emotionally drained and seriously considering leaving, which directly affects staffing and continuity of care.
So when we see these patterns around students and new nurses, we are not just dealing with clashing personalities. We are looking at a culture and safety issue that starts as early as the first clinical day.
Emotional Intelligence As A Clinical And Teaching Skill
A growing body of literature in nursing education has linked emotional intelligence with better stress management, communication, and relationships for both students and nurses. A recent review found that higher emotional intelligence was associated with improved coping, stronger interpersonal skills, and more effective teamwork, and that targeted training could strengthen these skills in nursing learners (Dugué et al., 2021).
EQ is not extra. It is part of safe, practice-ready nursing. For nurse educators and preceptors, emotional intelligence becomes both a clinical skill and a teaching skill. Each time we choose to pause instead of snap, to name what we are noticing instead of ignoring it, or to give feedback in a way that protects dignity, we are modeling a different way of being a nurse.
From Problem to Practice: A Quick EQ Snapshot
If you want a simple way to bring this into real life, start with the visual guide below, Incivility in Nursing: How Emotional Intelligence Turns It Around. On the left are six common behaviors that show up in education and practice. On the right are emotionally intelligent responses that draw on self-awareness, empathy, social awareness, self-regulation, conflict management, and relationship-building.
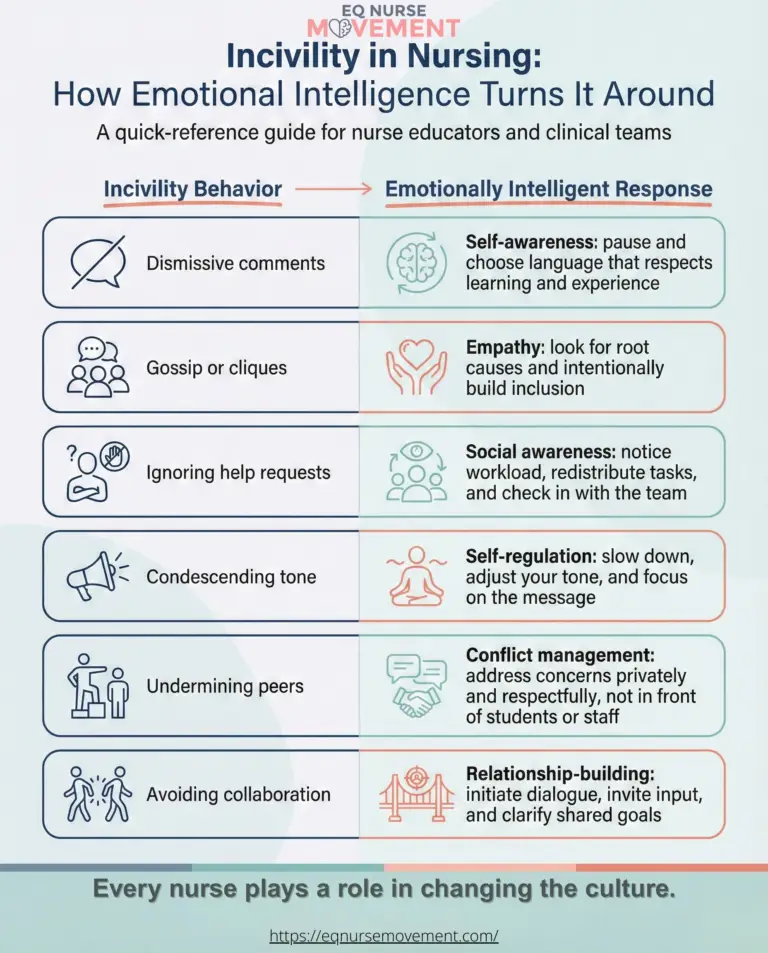
You can share this with students, preceptors, and faculty, or keep it where you prep for class or clinical as a quick reminder that every nurse plays a role in changing the culture.
Bringing This Into Your Work
If you are already maxed out, the goal is not to launch a big initiative. It is to change a few everyday reflexes.
You might start here:
One micro-practice for you.
Choose a simple habit, such as taking two slow breaths before responding when you feel irritated or rushed, or silently naming what you feel and what you want for the learner. Use it in the moments that usually trigger you.
One question for students.
Add a single question about emotional climate to post-clinical debrief or lab. For example, “Did anything today feel dismissive or unsafe, even in small ways?” Thank students when they name something.
One conversation with colleagues or preceptors.
In a huddle or meeting, name a few subtle behaviors you have been noticing and ask, “Do any of these feel familiar here? When you see this with a student or new nurse, how do you usually handle it?” Listen for what is already working and where people feel stuck.
None of this requires a new policy or committee. It is about building awareness, language, and small shared practices that make it easier to protect learners and keep patients safe.
Conclusion: Modeling the Culture They Deserve
Most of us can remember a time when we were the student or new nurse who stopped asking questions. Many of us were told that was just how nursing is. Toughen up. Get through orientation. Then you can relax.
You are not the problem. The system needs to change, and nurse educators are in a unique position to start that change.
Emotional intelligence will not erase incivility overnight. It will give you a way to see it clearly, name it honestly, and respond in ways that protect learning and patient care. One interaction at a time, you are modeling the culture your students and new nurses will carry forward.
One aligned action. Choose one interaction, one micro-practice, and one learner to protect. That is enough to begin.
Key Takeaways
- Incivility in nursing is often quiet and subtle, but it strongly affects psychological safety, learning, and patient outcomes.
- Early experiences of incivility shape professional identity and a learner’s belief about whether they belong in nursing.
- Emotional intelligence is a clinical and teaching skill that supports more thoughtful responses to incivility in real time.
- Small habits, like pausing before responding or asking one honest question about safety, can begin to shift the culture in classrooms and clinical settings.
Reflective Questions for Nurse Educators
- When was the last time you saw a learner “shrink” after an interaction on the unit or in class? How did you respond, and what might you do differently next time?
- What messages about “who belongs here” are students and new nurses receiving in your current setting, especially on busy or stressful days?
- Which emotional intelligence habit feels most realistic for you to practice this month: pausing, naming what you feel, or changing the way you give feedback?
References
Alsadaan, N., Ramadan, O. M. E., & Alqahtani, M. (2024). From incivility to outcomes: Tracing the effects of nursing incivility on nurse well-being, patient engagement, and health outcomes. BMC Nursing, 23, 325. https://doi.org/10.1186/s12912-024-01996-9
Dugué, M., Sirost, O., & Dosseville, F. (2021). A literature review of emotional intelligence and nursing education. Nurse Education in Practice, 54, 103124. https://doi.org/10.1016/j.nepr.2021.103124